Don't you hate searching for things?
PERIOPERATIVE EQUIPMENT
Aim: To provide an opportunity to gain knowledge and understanding of operating suite equipment. Offering a high standard of expertise regarding the safe and correct functioning of this equipment.
Electrical equipment
Basic safety guidelines:
1. All electrical equipment should be routinely checked and tagged by appropriately qualified personnel on an annual basis and by staff prior to and after each use.
2. All electrical cords should be inspected for imperfections, tears and kinks should be noted, taken out of use and sent for repair and/or a replacement ordered.
3. The use of extension cords should be minimised and kept of traffic flow area due to their potentially hazardous nature, ie. Avoidance of personnel tripping up and falling, keeping cords from lying in water.
4. All personnel should be instructed in the safe use of equipment used in the operating suite, inservice education should be provided regarding their function and appropriate
Use.
5. When equipment is found to be faulty, an understanding of the procedure to remove and repair is essential.
Electrosurgical Unit/Diathermy
The high-frequency current from an electrosurgical unit (ESU) is frequently used to cut tissue and coagulate blood vessels.
An ESU has output connections for both the active and dispersive electrodes. The unit should provide a sentry alarm that will detect incomplete circuits; one for the active electrode (cable contact) and one for the dispersive electrode (patient contact).
The active electrode - delivers the power to the operative site and can be activated by either hand or foot control.
MONOPOLAR CIRCUIT
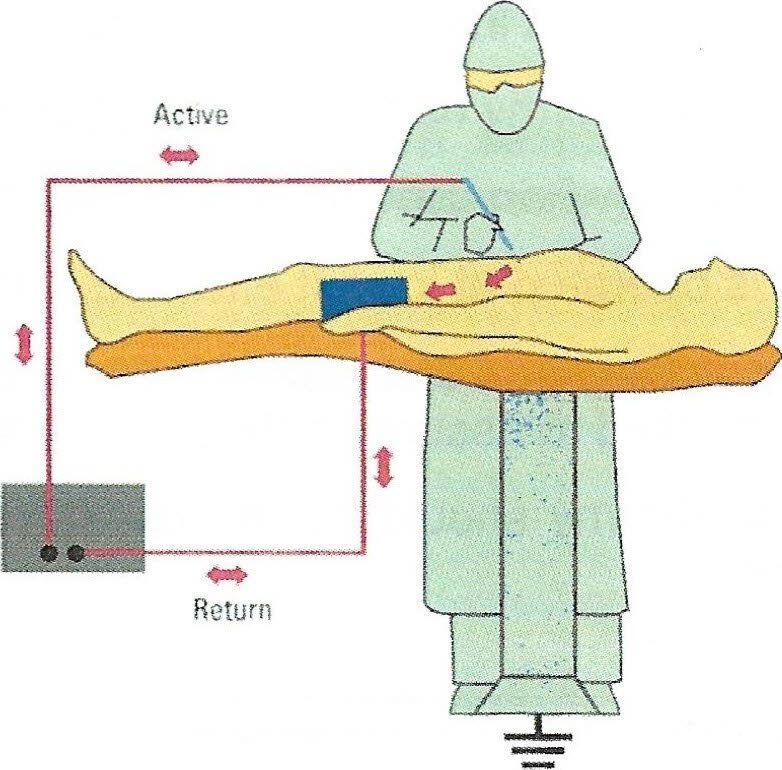
This picture represents a common monopolar circuit. There are four components to the monopolar circuit:
o Generator
Active Electrode
o Patient
Patient Return Electrode
The dispersive electrode - the ESU electric circuit requires delivery of the current via the ESC/ and active electrode. This returns to the ESU via the dispersive e/ectrode or patient p/ate. The functions of a dispersive e/ectrode are to provide a large surface area for the current to leave the patient, maintain low density, and reduce the temperature of the tissue, preventing a surface area burn. Modes of Delivery
Monopolar - The current flows from the ESU when activated by the surgeon either by a footpedal or handswitch. It originates in the generator and flows through the active electrode into the patient. The dispersive electrode (patient plate) then captures the current and returns it to the generator. Two types of monopolar coagulation are available, pinpoint and spray.
* Pinpoint - Use with forceps, all types of pencil electrodes, clamps and endoscopic devices. The technique employed is to contact the tissue or clamp, then activate. Pinpoint coagulation is intended for use on a small — defined area.
* Spray - Use with all types of pencil electrodes. A needlepoint electrode will overheat and fail at a high wattage setting. Do not use spray coagulation with a clamp. Spray coagulation can be used on all types of tissue whenever it is desirable to coagulate a lar er area.
BIPOLAR CURCUIT
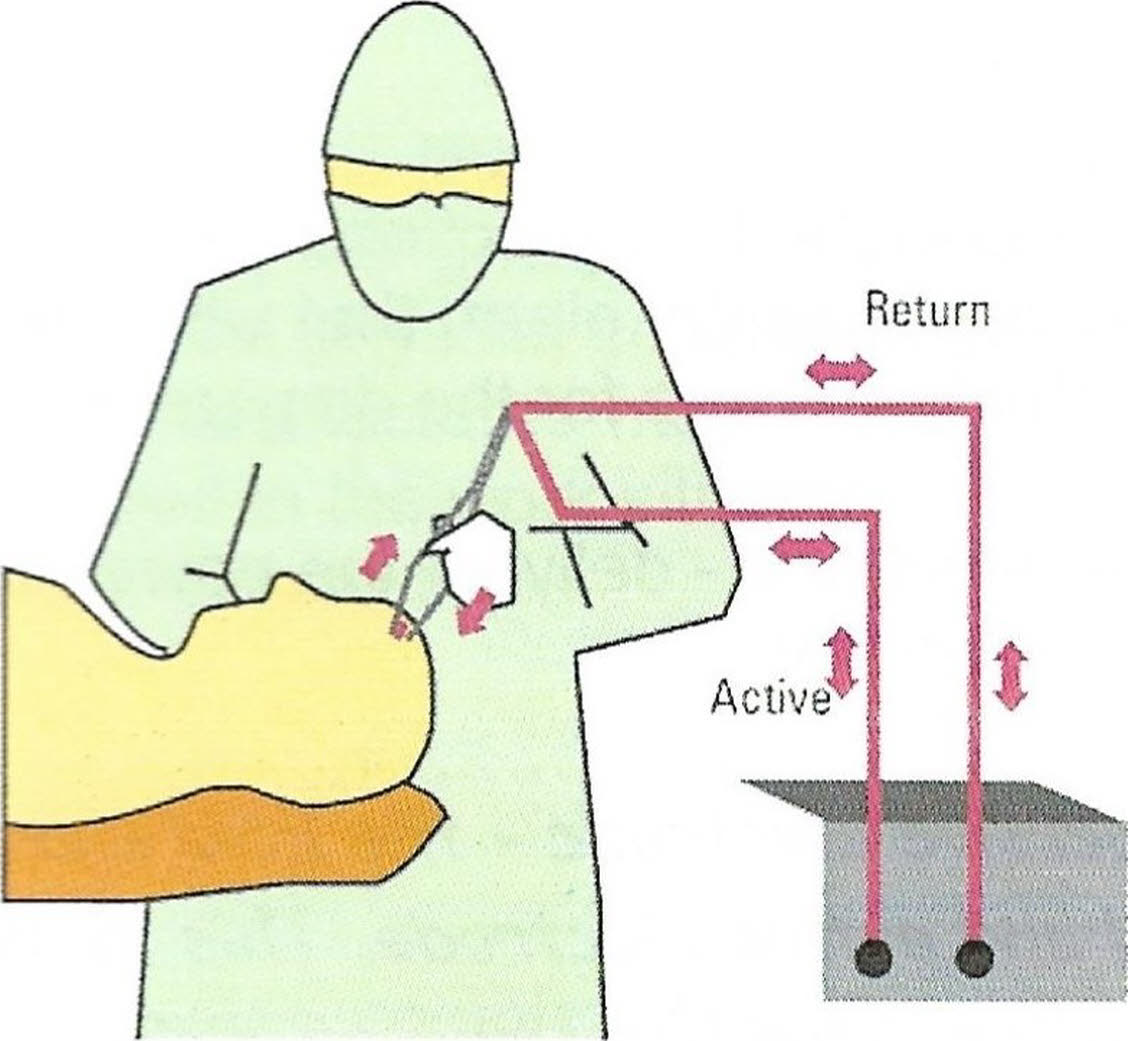
This picture represents a typical bipolar circuit.
If the patient has a pacemaker it is recommended diathermy should not be used. Should it be necessary a bipolar diathermy is used.
Bipolar - The active electrode is one tip of the diathermy forceps, the dispersive electrode the other. The power is distributed to a very limited area (Between the tips only). The current passes from one tip to another then along the diathermy cord and back to the machine. A diathermy plate is not required. The actual wattage power is reduced making it safe to use on delicate tissue, EG. Ophthalmology, neurosurgery and plastic surgery.
Use of Diathermy in Fluid
An increase in current is required when used in fluid. Glycine 1.5% should be used for longer procedures as the use of water may haemolyse red blood cells if sufficient enters the patient's circulation. An example of this would be a TURP, glycine should be used. Sodium chloride should not be used as it acts as a conductor and disperses the current. Gyrus Machine (Orange) also used for Large TURP only uses Sodium Chloride 3L bags. Please take note what machine the Dr is going to use. Ask the Nurses in that theatre!
Safety Requirements
* Test Cord fault alarms
* Inspect all accessories and cables for damage and excessive wear, including insulation on laparoscopic instrument sheaths.
* Ensure diathermy handpiece (electrode) is always kept in the quiver when not in use.
* Foot pedal, when used, is covered with clear plastic to keep it dry (if necessary).
* ESU is operated at lowest effective setting.
If re-positioning of the patient is required after placement of the ground pad, ensure plate is rechecked to assure continuing contact.
The diathermy should not be used in the presence of flammable agents, EG; Acetone, alcohol.
The light source has an adjustable brightness control that can be manually or automatically_ set. The automatic setting will adjust itself according to the image, requiring less need for any adjustment during the procedure.
The light source will require the bulb to be changed intermittently. These are usually easy to replace. The bulb should never be handled directly as it may be very hot and the oils on your hand may adhere to the bulb causing it to burn out quicker.
Endoscopic Equipment
Fibreoptics are used in endoscopy procedures, performed either in surgery, the ICU site, through a natural opening in the body (eg. bronchoscopy, colonoscopy or cystoscopy) or through an artificial opening created via an incision, such as an arthroscopy or laparoscopy. Additional types of endoscopic procedures can be performed during a surgical procedure for example, a choledochoscopy during a gallbladder procedure, or a nephroscopy during surgery on the kidney. Although each piece of equipment is unique and serves a specific purpose, all endoscopic equipment has similar working parts.
Camera Systems - Basic Components:
* Scope
* Coupler
* Camera Head
* Camera Controller
* Monitor
* Light Source
* Light Cable
All seven components must be operating properly to achieve an optimal image. If problems occur, always notify the relevant company so that repairs or adjustments are done quickly.
Fibreoptic Headlight
A fibre-optic headlight is used whenever the surgeon requires a highly intense light into a small area such as the throat, ear, nose, or deep cavities.
The headlight has a cord attached to it, and is usually positioned on the surgeon's head prior to the scrub procedure, Once the gowning procedure is finished the circulator will attach the headlight to light-source and increase the intensity as required.
Care
Treat the fibre-optic cable with care to prevent breakage and to prolong its' life. Examine cable for damage, When storing the cable, let the memory assist the coiling of the cable.
Safety
Never place the exposed distal end of the fibre in direct contact with flammable materials while the illuminator is operating ie. Never rest the cable on drapes.
Never point the distal end of the fibre directly at the eye when the unit is operating. The brilliant light output can cause eye injury.
The Operating Microscope
Allows the surgeon to examine a magnified area upon which more precise surgery can be performed. It consists of four basic components:
- An optical lens with controls for magnification, illumination and focusing.
- A mounting system for stability.
- An electrical system.
- Accessory items/attachments.
Optical Lens System
The lens system is the 'eyes' of the microscope, which consists of the objective lens and attached to the body are the binocular oculars or eyepieces, through which the surgeon views the image. This lens is interchangeable allowing for exact visualisation of the surgical field.
Magnification
The oculars serve as magnifying glasses that can assist the surgeon in obtaining a sharp non-distorted image. Each eye may require different magnification; both oculars can be adjusted separately until a clear picture is visualised (stereoscopic vision).
Light Source
Illumination of the area to be viewed is most commonly transferred through a fibre-optic cable, known as a co-axial illumination. Like all electrical equipment, safety and maintenance are essential to its optimal usage. Light controls should be set in the 'off' position when turning the microscope on and off to avoid short circuiting the unit.
Focusing
This can be accomplished manually or by the foot control piece. It will raise or lower the body of the microscope. Focus of the ocular lens should start at zero and be adjusted as required. The placement of the foot control should be announced to the surgeon so he/she is aware of its location.
Sample text simply exists so you can see what your new block looks like. To replace the text click on it and press CTRL+A on your keyboard to select the text. Then enter your own text to replace it. Our beautiful content blocks make creating great looking websites easier than…
The Floor Stand
Provides portability and stability. It is mounted on 5 twin castors. A spirit level allows accurate levelling, adjustment of the 'brakes' or feet can allow for the unevenness of the theatre floor.
The Column
All the electrical components are housed in the column. Two handles permit ease of movement of the microscope. The controls are arranged at the upper end of the column. They are colour coded to match the function outlet plugs.
The Articulated Suspension Arm
Has an adjustable spring tension allowing for counter balance of the microscope. The motion resistance of all joints is adjustable so that the arm can be secured at any height.
Assistants' Binoculars
An additional pair of eyepieces/binoculars can be mounted and used by the assistant/scrub person. This can be accomplished, however, with a beam splitter and an observer tube. The microscope should have the required optics in place prior tot the commencement of surgery.
Mobile Stool
A cushioned chair/stool should be available for the surgeon and scrubbed personnel as required. The chair may be draped to prevent less chance of the sterile field being contaminated.
Special Considerations
Unscrubbed Personnel's Responsibilities:
1.Check to see that all knobs are secured after the microscope has been placed in the final position.
2.Assist the surgeon with attachments of accessory items.
3.Take special care of power cables to prevent accidental breakage; position them out of the path of the microscope; be sure they are properly coiled for storage.
4.Take special care of the lenses to avoid breaking, scratching, or leaving fingerprints; tighten to finger tip tightness only, being careful not to cross-thread during attachment. When attaching the lens, perform the task over a padded surface to prevent accidental breakage if dropped.
5.Keep extra lamp bulb and fuses available and know where to find accessories and anticipate their usage depending on the proposed procedure and/or surgeon's preference.
6.When moving microscope, position the viewing portion over the base to add stability; acquire adequate moving help to accommodate the move safely.
7.Cover foot pedal with a plastic bag to keep dry and clean, and position it for easy access after surgeon has been seated or has determined desired position to perform surgery.
Scrub Persons' Responsibilities:
1.Verify with the circulator/surgeon the lens and binoculars for the specific procedure/surgeon.
2.Make sure lens and oculars are clean.
3.Have appropriate drape/handles to accommodate microscope accessory_ items; know how to apply the drape /handles correctly, using aseptic technique.
4.Put the mayo and instrument table in a convenient location (If assisting) so eyes do not have to leave the field to look around the microscope.
5.Maintain a calm atmosphere; know that dissection may be slow and tedious. Try not to let your attention stray.
Maintaining Body Temperature for the Surgical Patient
A common hazard for perioperative patients is hypothermia. This can result in less positive patient outcomes possibly leading to impaired wound healing, increased risk of wound infection, increased bleeding, and other physiological events, ie. Ischaemia.
During a surgical procedure heat loss may occur from-
The operating room (OR) temperature.
1.The type of surgery.
2.The length of surgery.
3.The patients pre existing condition/age.
Interventions to reduce heat loss intra operatively:
4.Increasing OR temperature.
5.Keeping patient warm pre and post operatively.
6.Use a forced air- warming blanket.
7.Warming irrigation solutions.
8.Warming intravenous fluids.
Radiation Safety
The use of radiation in the operating suite presents a potential hazard for patients and staff. Exposure to radiation can have long term dangerous effects on the body therefore exposure should be kept to a minimum or avoided if possible, The surgical team should wear protective gowns and accessories.
Types of Intraoperative X-Rays
X-rays for identifying and positioning ie. Ambi hip
Diagnostic studies — intra-operative cholangiogram o Emergent procedures — trauma, foreign bodies ie. Loss of a suture
Types of X-Ray Equipment
1.Fixed X-Ray.
2.Portable X-Ray.
3.Image intensifier.
4.Radiopaque contrast medium.
Radiopaque Contrast Medium
This substance allows for the visualisation of internal structures. A lot of these contrast mediums are made up of iodine. A patient's allergy status should be noted for any iodine, shellfish based sensitivities, as reactions can be potentially fatal.
Contrast medium may be diluted or undiluted according to the surgeon's preference. It should be diluted with sodium chloride if necessary.
Interventions To Decrease Risks While Using Radiation
1.Maintain distance from the radiation source.
2.Protective lead aprons, thyroid shields, and other accessories should be applied before scrubbing.
3.All unscrubbed OR personnel should leave the room during intermittent screening. If necessary unsrubbed team members required to stay in the OR must don a lead apron or use a lead screen to stand behind.
4.The incision should be covered with a sterile drape and the C-arm or X-Ray cassette should be encased within a sterile drape.
5.A radiologist must always be in attendance when the X-Ray is in use.
6.Pregnant personnel should not be exposed to radiological procedures.
7.If radiation-monitoring devices are available the badge should be worn on the outside of the lead apron. These badges are usually collected at specific times and data collated regularly to avoid excessive radiation exposure.